


This promotional material is intended for UK Healthcare Professionals only.
BOTOX® (botulinum toxin type A) Prescribing Information and adverse event reporting information can be found below.









How to diagnose post-stroke spasticity (PSS)
Diagnosis and treatment of PSS during the first 3 months post-stroke may benefit patients in their aim for a full recovery6, 7
It is possible to identify the functional risk factors that may contribute to the development of chronic spasticity.8

Dense weakness, sensory loss, light touch8

Visual impairment, cognitive loss, memory8

Proprioception, perception, neglect8
The PSS risk classification tool has been developed by a panel of experts and AbbVie to help spasticity patients get the timely treatment they need
The PSS Classification System was created with the assistance of a group of International experts in the field of PSS and AbbVie, utilising both published risk factors and their own clinical experience9
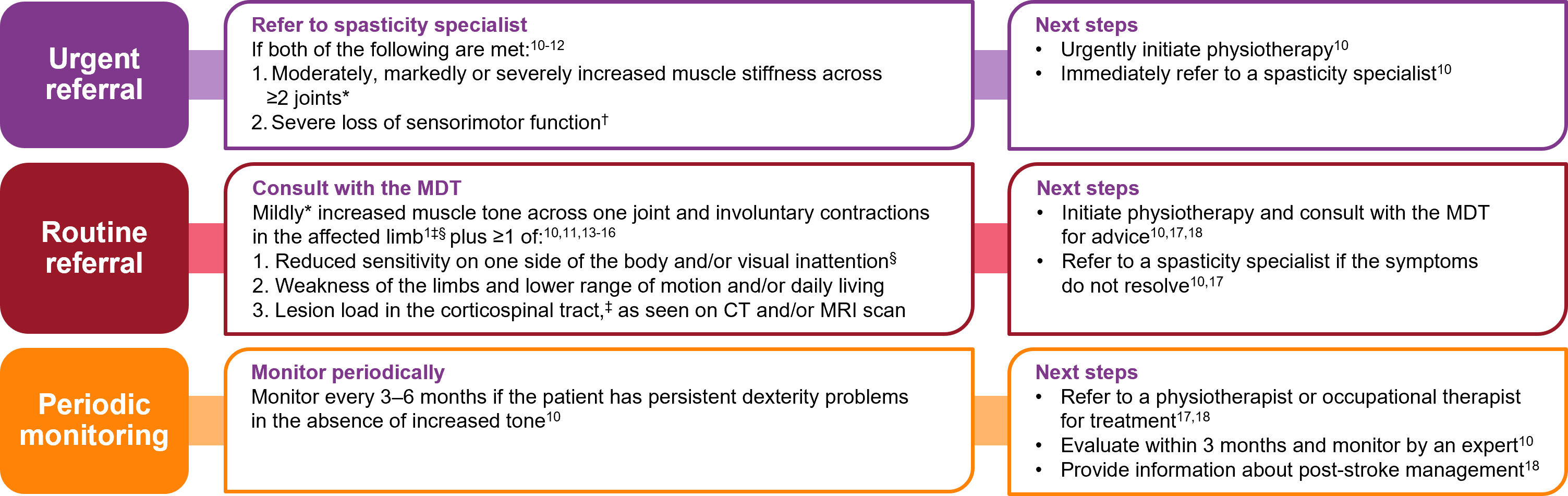
Figure adapted from Wissel J et al. 20209 and Bavikatte G et al. 202110
*Mildly increased muscle stiffness = Modified Ashworth Scale (MAS) 1 or +1; moderately = MAS 2; markedly = MAS 3; severe = MAS 4.19 †Measured using the Fugl-Meyer Upper Extremity Scale.12 ‡Muscle contractions should be differentiated from contractures. §Visual inattention includes hemianopsia, scotoma or visual neglect. **Can be measured with the Barthel Index (low score) and EQ-5D (low score).11
Possible additional risk factors for the development of post-stroke spasticity include:
- smoking (defined as current and past smokers)11,13
- left-sided stroke11
- enhanced manual activities prior to the stroke11
CT: computerised tomography; EQ-5D: EuroQol-5D; MAS: Modified Ashworth Scale; MDT: multidisciplinary team; MRI: magnetic resonance imaging; PSS: post-stroke spasticity.
By clicking the link above you will leave the AbbVie Pro website and be taken to the eMC PI portal website.
Adverse events should be reported. Reporting forms and information can be found at https://yellowcard.mhra.gov.uk/ or via the MHRA Yellow Card app, available in the Google Play or Apple App Stores.
Adverse events should also be reported to AbbVie on GBPV@abbvie.com
Date of preparation: June 2025. UK-BTX-250071.
